Yesterday, I was extremely privileged to be invited to an event INSIDE Parliament! Mothers for Mothers were celebrating their 45th birthday and the launch of their report: This Is Our Truth: A Grassroots Call to Reimagine Perinatal Mental Health Care. You might remember the adverts on here for it, or even have taken part in their survey some months back…?
It was somewhat surreal day for little old me! I had a formal invite and everything, and instructions to bring photo ID. Because I arrived a bit early, I made sure to visit the statue of suffragette Millicent Garrett Fawcett first. I then queued up behind a gaggle of excited primary school kids at the main visitor entrance.

After showing my invite and ID and being ushered through airport-style security, I was surprised to just be given a visitors pass and left to make my own way to the Churchill room for the event!? Security guards were extremely friendly and helpful at showing me the way, though. Bless. They were even high-fiving the school kids.

But what was this all for?
This Is Our Truth: A Grassroots Call to Reimagine Perinatal Mental Health Care
You can read the full 92 page report here.
They were spot on to call it “This is our truth”. The voices of lived experience are quoted extensively throughout. I always find this the very best way to make any research or data more human. It’s important to remind decisionmakers that every snippet of data represents an individual / family, whose life experience matters!
The length of time I waited — nine months — is far too long after such a significant trauma. There is nothing in the community that would understand what we went through… and so really that high level professional support needs to come sooner.
Quote from a respondent
The researchers sought out and brought together the experiences of 791 women and birthing people. They also got feedback from 56 VCSE organisations (Voluntary, Community, and Social Enterprises – like Big Birthas). Collectively, this represented 23,000 voices. The truth they tell is painfully familiar: mental health care in the UK during the maternity and post-birth period is still a postcode lottery, still too reactive, and leaving far too many families to cope alone.
One in Four
The report opens with some stark reminders:
Every year in England, around 600,000 women give birth. 26% will experience perinatal mental illness; that is, around 156,000 women and birthing people annually. Yet of those, only 57,000 receive specialist services.
Families describe services that are overstretched, rushed, and inconsistent. The long waits and short appointments leave little room for honest conversations about mental health. Services are under‑resourced, mental health is not seen as a priority (as we’ve seen in our own Wellcome-funded research), support available is reactive, not proactive – and usually only becomes available when the family reaches crisis point.
None of this is rocket science. None of this is anything revolutionary – we’ve been saying it (along with many others!) for a long time.

The report also challenges the persistent myth that parents “hide” or “underplay” mental health symptoms. Many do speak up – Big Birthas members have raised this before too! For various reason we are dismissed, told that it’s not important ‘right now’, something is more pressing (usually in our case, our BMI). Or we don’t meet the threshold for help. Or we fear judgement, child removal, or having concerns written in our notes. Often it’s not reluctance; it’s self‑protection in a system that doesn’t always feel safe.
Positive experiences often came down to trust, continuity and compassionate communication. Negative experiences; feeling judged, dismissed, or not listened to, can have long‑lasting emotional effects and make people less likely to seek help again.
The Bigger Picture
Mental health is shaped by wider life pressures. Being pregnant and having a baby is life-changing and daunting enough. That’s before you take the mental torture that is sleep deprivation into account!
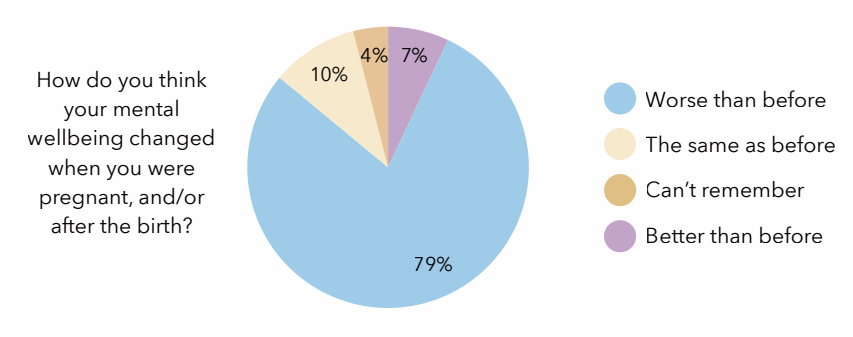
Even allowing for the fact that people likely to complete a survey about mental health are probably more likely to report an issue, having nearly 8 out of 10 respondents saying that their mental wellbeing worsened over this period… That’s really quite shockingly high.
Challenges such as financial stress, relationship difficulties, feeding problems, housing insecurity and bereavement all affect mental wellbeing too. There can be multiple challenges. Unsurprisingly, parents in the survey overwhelmingly said they wanted holistic support, not just clinical treatment. And, as the report highlights:
There are a lot of health care practitioners who see the problems but there is not the help or resource out there to do anything about it.
Support needs to be more personalised. The standard services that exist (where they DO exist) aren’t equipped or resourced to cope with the varied circumstances and experiences of the people who need them.
How VCSE Organisations (like Big Birthas) fit in
NHS provision is currently full of gaps, with voluntary and community sector organisations doing their best to catch and support families who fall through. But they’re doing it while juggling rising demand, increasing complexity, and unstable funding.
Big Birthas is a tiny organisation. We have never received any form of formal funding in the 15 years it has been running. The tiny amount of advertising covers maybe 5% of the annual costs of hosting the website, and that’s it. The rest I pay for myself out of pocket.
There’s no staff, no infrastructure. And so, I’ve never offered any more formalised support through Big Birthas than the Facebook Group and website, despite there being a need for it, because I can’t fund it. I’m not even able to update the site as much as I’d like, because it’s time consuming to do. I could hardly expect anyone else to want to do it for free, either! Luckily the Big Birthas community is really self-supporting – and I have some amazing volunteer admins on the group to assist on the rare occasions intervention is necessary. It’s a lovely space and I wish it had existed when I needed it. When I started BigBirthas, that was one of the few ambitions I had!
The precariousness of short-term funding…
I could have applied for grants to do more, its true. But I’ve worked for charities, and the constant churn of seeking, then applying, then reporting on short-term funding for services was a Sisiphean task I wasn’t prepared to start, or manage! Funders only seem to want to support new projects, and then only for a maximum of 3 years. Just as a project is getting into its groove, it’s time to start winding it up again!? Meanwhile, people who need the services are let down, confused, and often become disenfranchised. Besides, I never found the time to apply for Big Birthas to become an official charity or even a CIC – though it was originally one of my aims!
But this is the reality of VCSE organisations up and down the country. They’re supporting women and birthing people and their families, often on a complete shoestring, doing vital work in extremely precarious circumstances. They need and deserve long‑term investment, not short‑term scraps.
How I’ve chosen to further BigBirthas work instead…
With Big Birthas in recent years I’ve consciously pulled back from finding and supporting individuals with their trauma (much as I’d like to!) because I simply can’t satisfy all the need that exists singlehandedly. I’ve also pulled back on the website – I’ve focused my efforts less on chatty blog posts that may have been fun to read, and were good for visibility on search engines, but weren’t breaking any meaningful ground. Others have also moved into this space, offering information and support, there’s even several books available now! So I feel less like I’m leaving anyone in the lurch.
I concentrate exclusively now on communicating just essential updates about relevant news and research, and post much less frequently. Of course, this means Google is less likely to suggest the site to people… I’ve just checked today, and if you type ‘Plus size Pregnancy UK’ into Google – we’re way, way way down the list of results these days. We used to appear around 3rd or 4th! All the effort I put into getting up to the top of results doesn’t last if you don’t keep it up… But c’est la vie. Instead, I’ve looked to use my limited time in a different way.
Tackling the root cause
For at least the past 5 years, I’ve been working hard instead on getting my feet under the right tables and talking about the issues in the right rooms to the right people. I’m doing whatever I can whenever and wherever I can. And given that Big Birthas isn’t my job, I’ve been pretty busy:
For 3 years, I was a lay member for the NICE guideline committee on Maternal and Child Nutrition and I now sit on the MHRA Womens Health Expert Advisory Group. I’ve been on steering groups on several topics for the Royal College of Midwives and the Royal College of Obstetricians and Gynaecologists.
I lecture annually for a number of Universities on their midwifery, social care, and psychology courses – speaking about patient experience and higher BMI care – trying to get the word in early with new recruits about the importance of non-judgemental, compassionate, person-centred care.
I’m also regularly involved in PPIE (Patient and Public Involvement) in various research spheres – I sit on steering groups for the National Perinatal Epidemiology Unit and the Birth Options study, among others, along with helping individual research projects from time to time – making suggestions on study design, recruitment, publicity, wording, ethics, graphics, reviewing journal articles – anything really! I’m happy to help researchers who request my input however I can, and luckily funders now expect this level of involvement from people with lived experience, so it’s becoming more and more normalised.
Our voices deserve to be heard!
And if professors/gynaecologists/obstetricians/midwives slip into using stigmatising language, or make assumptions based on outdated, ill-informed, or judgemental attitudes, I’m ready to prod them with a big (metaphorical) stick and point them in the right direction.
My focus has been on targeting the root causes of perinatal trauma for people with higher BMIs. Getting the policies, guidelines, training, staff, managers, and research on side. And not just for those of us in bigger bodies, but for all women and birthing people. People making important decisions that affect our lives need to hear our stories and our voices! It’s why I’m always urging readers of this page to get involved with research.
As one of the speakers said yesterday:
When people experience traumatic events in pregnancy, it’s entirely reasonable to expect mental ill health as a result. But when thousands of women and birthing people every year are experiencing trauma and subsequent mental ill health as a result of pregnancies/births where there was no significant adverse event that caused it – merely as a result of the way they are treated by the system – we have to seriously look at and change what is going on.
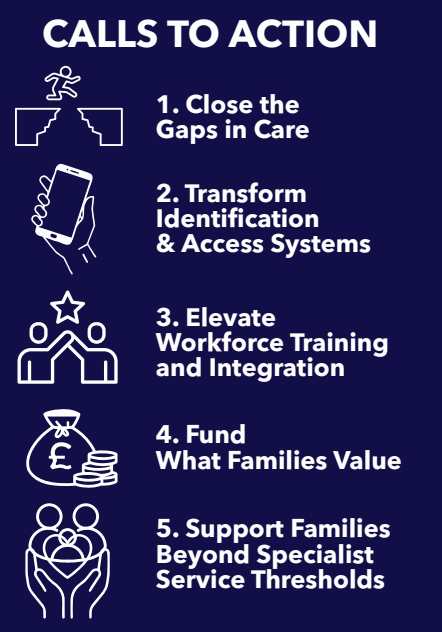
Mother for Mother’s five Calls to Action are clear:
I really appreciate the Mothers for Mothers report. They have been doing amazing work supporting people (wherever they can find funding to do so!), but in the long run, they’re right. We need to do what we can to change the system so people don’t NEED those services in the first place.
What makes this report so compelling is its refusal to separate mental health from the realities of life: housing, money, racism, trauma, feeding struggles, sleep deprivation, and the sheer emotional labour of early parenthood. It argues for holistic, personalised, relational care, not tick‑box checklists or crisis‑only responses, and it centres the voices of those who know best throughout.
I really hope the right people with the ability to affect real change are listening.