When you’re pregnant, one of the biggest decisions you’ll make is choosing where to give birth.
If you have a higher BMI, you might find that the conversation feels more medicalised, more cautious, and sometimes more limiting. Even if you’re not outright being TOLD you can/must do something, it often feels like you’re being herded into one specific pathway. But here’s the thing: you still have choices, and understanding your options and their pros and cons is the first step to making a decision that feels right for you.

Where should I give birth?
I cannot say this often enough. The RIGHT place of birth is the one that feels right to YOU.
Remember – vaginal birth and labour is overwhelmingly a physiological process. We’re mammals, at the end of the day, and your body has evolved to do this! But if you don’t want to birth your baby this way – that’s equally fine and valid choice too. There’s no gold star award for those choosing the most “natural” option, or the most “medical” one!
Don’t get me wrong – the baby has to come out one way or another! But for clarity, this article is about choices for those planning for a vaginal birth. I have a page on ceasarean birth here.
So what are your birthplace options?
There are (broadly speaking) 4 main options available to people in the UK planning a physiological birth. Though this very much depends on where you live, as not all options are available locally to everyone:
Home birth
What it says on the tin! Giving birth in your home (or someone else’s!). If there are any complications, you will be advised to transfer to a hospital setting ASAP. Some equipment options and pain relief (e.g. birth pool, gas and air (Entonox), pethidine), might be available, but not all. Your right to insist on a home birth is absolute, and protected by UK law. But while you have the right to, the NHS is not legally guaranteed to provide a midwife at your home. It is possible to hire a private midwife in the UK for personalised, one-to-one maternity care. Costs for an Independent Midwife typically range from £4,000 to £8,000.
Some trusts are supportive of home birth for people with BMIs over 30, particularly if there are no other complications, and especially when it’s a second or subsequent pregnancy and previous pregnancies have been unproblematic. Others may advise strongly against it and be very difficult. Knowing the situation locally is key! Ask around, check Trust websites for info. Submit Freedom of Information requests so you know the lay of the land.
Midwife-led unit (birth centre) at a different site to a hospital maternity unit (aka FMU or Freestanding Maternity Unit)
Intended as a home-away-from-home environment, staffed by experienced midwives, but no doctors onsite. Often with beautiful spa-like rooms, usually with pools, sometimes with double beds and other comfortable additions like twinkly lights that you wouldn’t expect in a hospital setting, but with the cleanliness you would expect of a hospital setting! Sometimes partners can even stay overnight with you.
These can be a great middle ground – less obviously clinical, but still staffed by professionals. Sometimes they are on a hospital site – just not one that has a maternity suite, but they can be on Industrial Estates, or somewhere else you wouldn’t necessarily expect! Again, not all pain relief or equipment options will be available here (no epidurals!) If there are any complications, you will still be advised to transfer to a hospital setting ASAP.
Some FMUs have BMI cut-offs, often around 35–40, (usually citing equipment limits or emergency considerations that can often be debunked, but I won’t get onto that soapbox here!) but more likely will assess you on an individual basis regarding potential admission.
Midwife-led unit (birth centre) at the same site as a hospital maternity unit (AMU or Alongside Maternity Unit)
Similar to the Freestanding units, but with one subtle and important difference. They’re on the same site as a hospital obstetric unit – often the floor above or below the Labour Ward/Delivery Suite, or just down the corridor. The huge advantage of this is obviously the proximity to doctors. If you needed to see a doctor, no ambulance needs to be called, and the travel time to get you onto the obstetric unit is extremely short.
Obstetric unit (hospital labour ward/delivery suite)
This is where you’re most likely to be recommended to birth if your BMI is higher, especially if there are other factors to consider.
This is what we tend to think of when we picture a ‘hospital birth’ scenario. You’re more likely to be labouring on a ward with other people, less likely to be in a private room, though you’ll likely be moved to a private room (delivery suite) when birth is imminent.
Here is where all the medical equipment is available, that means access to a greater variety of monitoring equipment, a greater range of pharmaceutical pain relief options and anaesthetics (e.g. epidural), instrumental birth assistance, and surgical care – along with nearby neonatal care if your baby is poorly and needs extra support. There will also be midwives – staff work in multidisciplinary teams, but overall decisions and control in what you are offered rests with doctors. But there’s no hiding that this is recognisably a hospital now – with all the noises, smells, and sights you’d expect. Whether that’s reassuring or offputting depends entirely on your own perspective!
Almost all obstetric units still have access to many of the ‘softer’ options for labour, e.g. aromatherapy, birthing balls etc. There’s usually a birth pool somewhere, but ask if it’s ever used if this is an important part of your pain relief plan – often, frustratingly, birth pools on obstetric units exist in name only and tend to be the room where spare equipment is stored, rather than a genuine offering!
What IS right for you?
Like any mammal giving birth, the conditions around us matter. Feeling safe, undisturbed, and supported can help labour flow, while stress, fear, or feeling observed or vulnerable can slow things down. Choosing a birthplace isn’t just about what might go wrong and guarding against it; it’s also about creating the conditions that help things go right.
There’s a few ways to think about this –
Do you find hospitals reassuring, or stressful?
Some people feel instantly safer knowing medical support is right there. Others find the lights, noise, and clinical environment make it harder to relax. There’s no right answer here, only the one that instinctively feels right for you.
In unfamiliar situations, do you like clear direction – or autonomy?
If you prefer being guided step-by-step, a more medical setting might feel containing and supportive. If you’re someone who likes to tune into your body and make your own decisions, a midwife-led setting (or home) might give you more freedom to do that.
How do you respond to risk?
Be honest with yourself here. Do statistics reassure you, or make your brain spiral? Any pregnancy, regardless of BMI is not without risk. Would you feel calmer knowing every possible intervention is immediately available – or more comfortable focusing on the (greater) likelihood of a straightforward birth?
How do you feel about the possibility of transfer?
With home birth and MLUs, there’s always a chance you may need to move to an obstetric unit. How far away is it? What would be the likely transfer time by ambulance? For some, it’s just “Plan B.” For others, it feels like a big unknown worry that would sit in the back of their mind and they’d rather start there and remove the uncertainty. Neither reaction is wrong – but it’s worth noting yours.
What support will you have around you?
While it’s your body and ultimately your choice, your birth partner’s attitude matters more than people sometimes realise. Will your partner feel calm, confident, and supportive in the different settings? Do they trust the process, or feel reassured by medical presence? Their energy can influence yours – so that impact is worth factoring in.
Practicalities and logistics
This is an easy one to overlook! Firstly, how far are each of the options from your actual home, how quickly can you get there, how reliably can you get there, and/or get between them, depending on time of day and time of year? If you’re thinking about home, are there animals or children that need to be accommodated? Is there room for a pool (if you want one)? Home births are surprisingly un-messy (at least in my experience – I was looking forward to a blood spatter up the wall I could point out proudly to future guests!) but you still might want to think about covering soft furnishings etc. and the practicality of the room and access that you’re planning to use.
What were your previous birth experiences like?
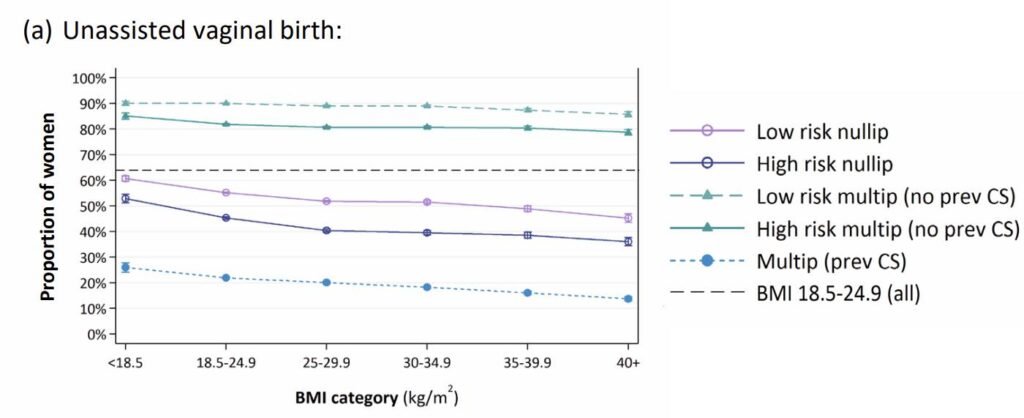
If this is your first birth, you’re likely a bit apprehensive – understandably! Around 40-50% of first births result in an unassisted vaginal birth, so you have very good odds of this happening.
If it’s a second or subsequent birth, you probably already have some ideas about how this one will go, and what you liked or didn’t like about your past experience. As a rule (though not always!) first labours tend to be longer. You might be surprised by how short the next labour will be in comparison, so that might also be an important planning component! (see The duration of spontaneous active and pushing phases of labour among 75,243 US women when intervention is minimal: A prospective, observational cohort study [2022])
If your previous birth was a vaginal birth, then the data from the RCOG BMI Over 30 Report is incredibly clear – your BMI is largely irrelevant – you have an 80%+ chance of another unassisted vaginal birth.
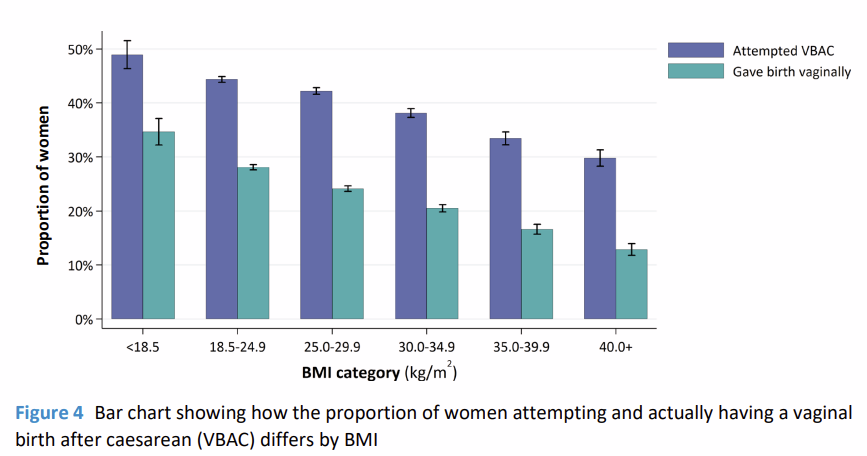
If your previous birth ended in a cesarean you hadn’t wanted, you don’t have to assume the same will happen again. While it is true that previous birthing experience is one of the best indicators of subsequent birth experience, the RCOG data also showed that around half of the people who attempt a vaginal birth after caesarean do give birth vaginally.
If you have been adversely affected by a previous birth and it’s really affecting your planning of this one, please do ask for support. Many trusts offer birth debrief or birth reflections meetings to help you – which many people report can be very helpful. There are also other organisations like the Birth Trauma Association who can help you access counselling if needed.
What kind of birth experience matters to you? Rank your priorities
Is your priority avoiding intervention where possible? Having access to pharmaceutical pain relief options? Being in water? Minimising transfers? Feeling at home? You don’t have to rank everything – but knowing your top 2–3 priorities can really help clarify what is important for you.
How has your pregnancy been so far?
BMI is just one piece of the picture. Your overall health, any complications, previous birth experiences, and how things are progressing all play a role. A personalised conversation with your midwife, or a consultant midwife/head of midwifery/supervisor of midwives about your own very specific circumstances can help translate guidelines and policy and options into what actually applies and matters to you.
What do guidelines actually say?
Guidance from UK bodies like NICE and the Royal College of Obstetricians and Gynaecologists (RCOG) is designed to support safe care, not to remove your autonomy. In the update to NG235 Intrapartum Care Guidelines in 2023, the committee looked at recent data and added a specific section about higher BMI birth, stating:
Impact of BMI on choice of place of birth
1.3.6 Advise women that, in general, the higher their body mass index (BMI) at booking (and particularly with a BMI above 35 kg/m2), the greater the likelihood of complications, so this may be something they wish to think about when planning their place of birth. Discuss with them that:in the event of complications arising, advanced care can generally be given more quickly in an obstetric unit or an alongside midwifery unit than at home or in a freestanding midwifery unit.
these complications include unplanned caesarean birth, postpartum haemorrhage, transfer from home to an obstetric unit, stillbirth, neonatal death or the baby needing neonatal care
the risk of complications may depend on whether the woman is nulliparous or multiparous, but in general the risks of complications are higher for nulliparous women with an increased BMI compared with multiparous women with an increased BMI
(Nulliparous = has never given birth before, Mutliparous = has given birth before)
This was a fundamental change from the previous blanket recommendation that we should all give birth in obstetric units. NICE absolutely recognise now that choosing where to give birth is our right, and we should have agency over it, and this is a very welcome edit. No longer is a midwifery led or home birth ‘Birthing Outside of Guidelines’ – with all the baggage that label brings with it! Hurrah!
Understanding the context (without the fear)
According to the most recent statistics (Child and maternal health profiles, December 2024 update: statistical commentary) more than a quarter of pregnancies (26.2%) now fit into the ‘obesity’ bracket. (Yup, we’re still using that word – click here for more info on BMI categories). By virtue of this, Trusts are becoming more experienced at ‘managing’ higher BMI pregnancies and being less fearful (and fearmongering) of us, our pregnancies, and our babies!
It’s true that a higher BMI is associated with increased chances of certain complications, such as gestational diabetes, pre-eclampsia, and a higher likelihood of caesarean birth. But statistics describe populations – not individuals. Most people with a higher BMI still go on to have healthy pregnancies and births. Many people do not develop any complications, and those that do have complications rarely experience negative outcomes as a result, since we can monitor and manage those complications well.
Yes, the risks are higher, but not by much. Conversations about risk should not overwhelm our pregnancy or our experience. Your experience is likely to be good!
Data on the various options for higher BMI pregnancies
Unfortunately, this is where we’re still lagging behind. Often when seeking data about birth outcomes and experiences for bigger women, we hit a brick wall. Almost always, the data concentrates on the experiences of ‘low-risk’ pregnancies, and excludes our experiences. So it’s really tricky to evidence safety and risk. e.g. in the use of pools for labour and birth, which have clearly been found to be just as safe as birthing on land – just not in people with higher BMIs!
This doesn’t mean that it’s not safe if you’re bigger. Indeed, it may be that it’s MORE safe – there’s simply not the data either way… and some clinicians really don’t like that uncertainty. Given that immersion in water is associated with some really useful advantages; ease of mobility, reduced blood pressure etc, I’m really hopeful that some research into higher BMI pool use in labour will be published soon!
The same is true of home births. There’s excellent data that for low-risk pregnancies in people who’ve birthed before, that a planned home birth is just as safe. Interventions are less likely, outcomes for the baby no different, but satisfaction scores are higher. Rates of vaginal birth are 3x higher in planned home births than in hospital settings, and have changed very little over the past few decades – whereas rates of ceasarean births in obstetric units have increased substantially!
Why is there a lack of evidence? And what does it mean?
For anyone who doesn’t fit into this very narrow band of labours and births that the current data has studied, the evidence is lacking. Again, that doesn’t mean these options have worse, better, or the same outcomes… It means we simply don’t know when the circumstances are different.
Even where researchers have expressly looked into the experiences of larger people, they’ve struggled to find the data. e.g. the UkMidSS ‘Severe Obesity’ Study into Midwife Led Unit Births, found that births in AMUs for those with a BMI of 30-40, without complications, who’d birthed before, had no worse outcomes when using a Midwifery Led Unit than people with lower BMIs. But there weren’t enough people in their study with BMIs over 40 for them to report on those with any degree of certainty.
The higher your BMI, the less available evdence there is on anything outside of birthing in a hospital obstetric unit. Your caregivers may not be able to provide you with information on risk specific to your cicumstances. If this lack of evidence bothers you, you might feel safer staying where higher BMI births generally happen – in hospital.
It’s not just about BMI
BMI is one factor in your maternity experience – never the whole story. Your overall health, previous births, mobility, and pregnancy progress thus far, all matter too.
Choosing your place of birth with a higher BMI is about balancing safety, comfort, and control. For some, that means the reassurance of a hospital setting. For others, it means advocating for a birth centre or home birth with clear planning.
Whichever path you choose, you deserve:
- Clear, evidence-based information
- Respectful, non-judgemental care
- A voice in every decision
Because this isn’t just about risk—it’s about your experience, your confidence, and your birth. One of the most life-changing and amazing experiences you can ever have.
And that matters.
This is about finding the environment where you feel safest, most heard, and most able to do the work of labour in your own way.
That’s the place where you’re most likely to thrive.
Good Luck – whatever you decide!
Big Birtha x